AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2690-8794/032
*Corresponding Author: Osman Demirhan, Department of Medical Biology, Faculty of Medicine, Çukurova University, and 01330 Balcalı-Adana, Turkey, GMS: 05060229765.
Citation: Nesrin Çetinel, Osman Demirhan, Mustafa Demirtaş, Çağlar Emre Çağlıyan, Aslıgül Cüreoğlu, İnayet Nur Uslu, Yaşar Sertdemir; (2020) The Genotoxic Effect of Interventional Cardiac Radiologic Procedures on Human Chromosomes J, Clinical Medical Reviews and Reports. 2(5);DOI: 10.31579/2690-8794/032
Copyright: © 2020, Osman Demirhan:. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 July 2020 | Accepted: 31 July 2020 | Published: 10 August 2020
Keywords: interventional radiology, angiography, coronary artery disease, cytogenetics, x-ray, contrast agents, chromosomal aberrations
In recent years, an important part of the ionizing radiation (IR) that human have been exposed for diagnostic purposes are interventional radiologic procedures. The X-rays and contrast media are used in angiography. The patients and staff members are exposed to X-ray during these procedures. While it is known that X-rays cause DNA damage and carcinogenesis, the effect of the contrast agent is still unknown. The aim of this study was to investigate the effect of X-rays and contrast agent on chromosomes of human patients. Peripheral blood samples were taken from 50 patients (30 males, 20 females, ages between 38-75 years). Chromosome analysis of peripheral lymphocytes in 50 patients were performed at 3 different periods; before the interventional radiologic procedure, 24 hours and 1-3 months after the procedure. Also, chromosome analysis was performed on 17 staff members working during interventional radiological procedures to investigate the effect of X-rays. Standard cytogenetic analysis techniques were used for this study. The frequency of chromosomal aberrations (CAs) was significantly higher in patients 24 hours after the interventional radiologic procedures than pretreatment (p=0,000). At the same time, CAs after 24 hours compared with those taken 1-3 months later, shown that the CAs were significantly reduced after 1-3 months (p=0,000). We also found that the frequency of CAs was also statistically higher in patients exposed to high radiation doses (p=0,042). Compared with the control group (n=30), CAs were found significantly higher in workers exposed to radiation. Our findings have shown that X-rays and contrast agents that used in interventional radiological cause chromosomal damage. For this reason, the dose of radiation to be given to the patient must be carefully selected. Due to the potentially high genetic damage of patients with coronary artery disease (CAD), the type and amount of medication to be given and the frequency of radiological diagnostic procedures to be performed should be meticulously adjusted.
Diagnostic ionizing radiation, such as X-rays are the largest man-made source of radiation exposure. The X-rays and iodinated contrast media are widely used for diagnostic radiology in angiography and in interventional radiology. Cardiac ionizing procedures expose both patients and medical staff to the highest radiation levels in diagnostic radiology. Exposure to IR may result in adverse health effect on patients and clinical cardiologists. There is a clear need to evaluate and establish biologic approaches for determining low-dose radiation effects in patients undergoing diagnostic X-ray procedures. Interventional cardiologists (ICs) are likely to receive high radiation exposure as a result of procedures they undertake. Unfortunately, many physicians are unfamiliar with radiation genotoxicity or the quantitative nature of the risks and IR risks are misunderstood. High radiation doses tend to kill cells, while low doses tend to damage or alter the genetic code of irradiated cells. Recently, as the number of diagnostic and interventional cardiac catheterisation procedures has greatly increased, serious radiation induced skin injuries and an excess of cataract development have been reported in exposed staff [1-3]. X-rays either acts directly on the DNA molecule or indirectly through the formation of reactive compounds that interact with the DNA molecule resulting in cytotoxicity of the cell [4]. IR can induce directly various forms of DNA damage, including the possibility of increasing the incidence of CAs and micronuclei (MN). CAs are the most fully developed biological indicator of IR exposure. It is widely accepted that there is an increased risk of cancer following exposure to IR; this is felt to be most likely due to damage to DNA strands during exposure [5]. However, a recent study has estimated that from 0.6% to 3% of all cancers are due to medical X-rays [6].
DNA double-strand breaks (DSBs) are the most relevant biologic damage induced by IR [7,8]. IR is uniquely energetic enough to overcome the binding energy of the electrons orbiting atoms and molecules; thus, these radiations can knock electrons out of their orbits, thereby creating ions. In biologic material exposed to x-rays, the most common scenario is the creation of hydroxyl radicals from x-ray interactions with water molecules; these radicals in turn interact with nearby DNA to cause strand breaks or base damage. The X-rays can also ionize DNA directly. Most radiation-induced damage is rapidly repaired by various systems within the cell, but DNA double-strand breaks are less easily repaired, and occasional misrepair can lead to induction of point mutations, chromosomal translocations, and gene fusions, all of which are linked to the induction of cancer [9]. IR can cause many types of DNA damage, in which DNA DSBs are most lethal, probably resulting in genomic instability and cause some diseases if unrepaired or misrepaired. Exposure of tissues and organs to IR can lead to cancer.
Despite all the above information, the aim of the present study is to investigate the effects of X-rays and contrast media on patients undergoing arteriography and interventional cardiologists.
The peripheral blood samples were collected by venipuncture from total 50 patients exposed to interventional radiological procedures (the X-ray and contrast medium) in the unit of angiography at the Department of Cardiology, Balcalı Hospital, Çukurova University, Adana, Turkey. The samples were taken: (1) before the procedures, (2) 24 hours after the examination and (3) 1-3 months after interventional radiological procedure in 25 patients. In the selected group of patients, 30 were males and 20 females, ranging in age from 38 to75 years (average age was 54, 31 years). In addition, the effects of the X-ray on chromosomes were investigated from 17 angiography workers (11 males and 6 females) occupationally exposed to the X-ray at the Balcalı Hospital, ranging in age 27 to 56 years and 30 individuals (17 males and 13 females) without any work-related exposure to ionizing radiation considered as control group whose ages ranged from 35 to 44 years. Informed written consent was obtained from all participants. The study was authorized by the Institutional Ethic Committee of Çukurova University.
Peripheral blood was collected into heparinised tubes from each subject for culture. Each sample was examined for expression of CAs in the Genetics Laboratory of the Department of Medical Biology and Genetics, Faculty of Medicine, Cukurova University. Lymphocyte cultures were set up by mixing 0.5 ml of whole blood samples, with 4.5 ml of PB-Max Karyotyping medium (Gibco). The cultures were incubated at 37oC for 72 h in an incubator, and colcemid (30 µl) was added 1, 5 h prior to harvesting. Standard cytogenetic techniques were used for harvesting and slide preparation. Three slides were prepared for each subject. The slides were prepared by trypsin GTG-banding and 50 metaphases/individuals were analysed on coded slides for structural CA, such as chromatid and chromosome breaks, deletions, acentric fragments, di-centric chromosomes, tetraploids, quadriradial exchange figures, and chromosomal exchanges. We conducted chromosome analysis using CytoVision software. Abberations were recorded according to the International System of Cytogenetic Nomenclature (ISCN).
SPSS 20.0 package program was used for statistical analysis of the data. Chi-square / Fisher Exact test was used to compare categorical measurements between groups. The Mann Whitney U test was used to compare the total irregularities without group distribution. The Wilcoxon Signed Rank test was used to compare pre-and post-treatment total irregularities without normal distribution. Statistical significance level was 0.05 in all tests. P values are given in tables with multiple comparison correction (Bonferroni).
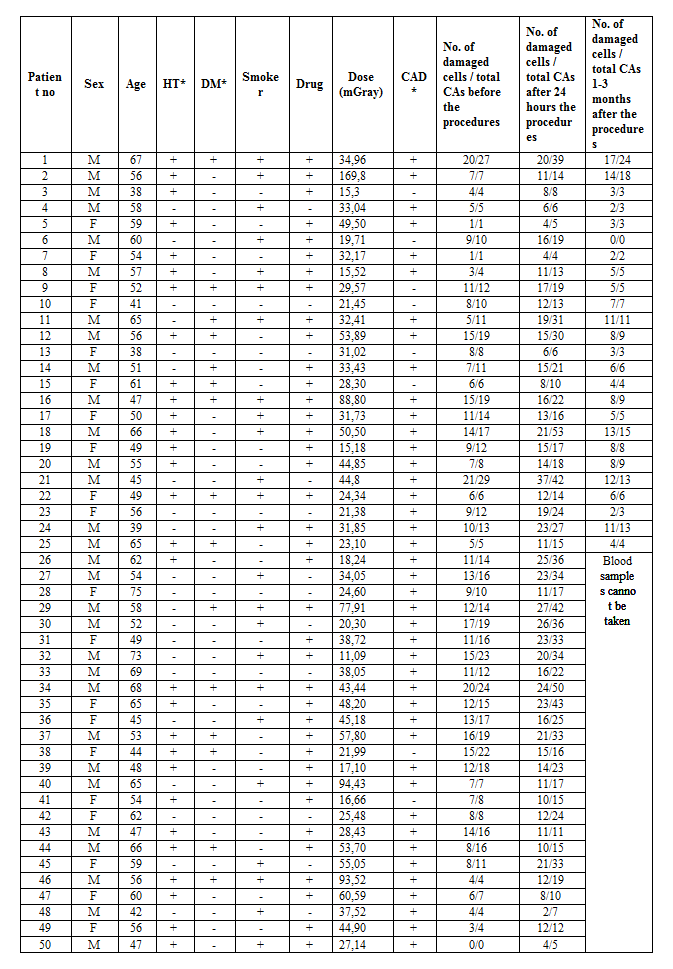
In our study; CAs occurred by analyzing 50 metaphase plates for each individual. Table 1 gives clinical, demographic characteristics and number of damaged cells for each patient.
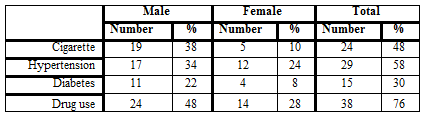
According to the clinical parameters (risk factors); 48% of the patients were smokers, 58% were hypertension, 30% had diabetes and 76% were using drugs (Table 2).
1. Chromosomal Abnormalities in Patients Before the Procedure
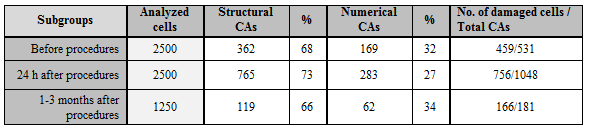
In this subgroup, 2500 cells were analyzed. One or more CAs were found in 459 of these cells. Total 531 structural (362, 68%) and numerical (169, 32%) CAs were observed (Table 3). Structural CAs were classified according to their significance; 27 (5,1%) deletions, 21 (4%) translocations, 2 (0,4%) duplications, 3 (0,6%) inversions, 20 (3,8%) chromatid breaks, 2 (0,4%) chromosome breaks, 8 (1,5%) dicentrics chromosomes, 2 (0,4%) neocentric structures, 238 (44,8%) fragile regions, 3 (0,6%) gaps and 36 (6,8%) 9qh+ chromosomes. Gonosomal chromosome mosaicisms; X chromosome loss was found in 3.5% (19 cases) and Y chromosome loss in 3.2% (17 cases) of the patients. XXXY was observed in one patient (0.2%), XXY in one patient (0.2%) and X chromosome in 4 patients (0.8%). Our study findings showed that X and Y losses mosaicisms were the most common chromosome aneuploidic mosaicisms in our patients. In addition, autosomal chromosome mosaicisms were observed in 3.9% (18 cases) of the patients. From these findings; autosomal monosomic mosaicisms (-20, -22, -18 and -21, respectively) were higher than autosomal trisomies (+21, +2, +8 and +18, respectively).
2. Chromosomal Abnormalities in Patients 24 hours after the procedure
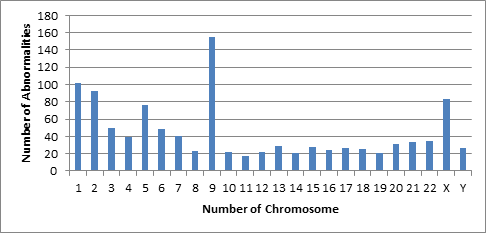
In this subgroup, 2500 metaphases were analyzed. A total of 1048 structural and numerical CAs were observed in 756 metaphases that including one or more various CAs (Table 3). A total of 1048 structural and numerical CAs were observed in 756 of 2500 cells examined (Table 3). These CAs were 73% structural and 27% numerical. Among the structural CAs; 6,8% (71) deletions, 3,7% (39) translocations, 0,3% (3) duplications, 0,7% (7) inversions, 0,2% (2) neocentric chromosomes, 0,4 (4) ascentric chromosomes, 0,1% (1) quadriradial chromosome, 4,1% (43) chromatid breaks, 0,4% (4) chromosome breaks, 1,1% (11) dicentrics chromosomes, 0,1% (1) isochromosome, 0,2% (2) ring chromosomes, 43,1% (476) fragile regions, 0,6% (6) gaps and 9,1% (95) 9qh+ chromosomes were found in the analyzed cells. In addition to observed structural CAs, 234 autosomal (22.3%) and 49 gonosomal (4.7%) numerical CAs were also detected. Among the gonosomal numerical CAs, 22 (2.1%) patients had X and 15 (1.4%) patients had Y chromosome loss, 2 (0.2%) patients had XXY and 10 (1%) patients had gonosomal chromosome mosaicisms such as +X [8] and +Y [2]. Autosomal monosomic mosaicisms (-22, -20, -21, -19 and -18, respectively) were higher than autosomal trisomic mosaicisms (+21). According to the findings obtained from the patients 24 h after the procedure the most affected chromosomes were 9, 1, 2, X, 5, 3, 6, 4 and 7, respectively (Figure 1).
3. Chromosome abnormalities at patients 1-3 months after the procedures
A total of 181 structural and numerical CAs were found in 166 defected metaphases of 1250 analyzed cells, at the subgroup 1-3 months after the procedure. The structural and numerical CAs were 119 (66%) and 62 (34%), respectively (Table 3). According to this findings, the proportions of fragilities, 9qh+, chromatid breaks, deletions, translocations and others were %42 (78), %8,8 (16), %6,6 (12), %3,8 (7), %2,7 (5) and %0,6 (1), respectively. Sixty-two (34%) numerical CAs were found of analyzed cells. Observed autosomal chromosome aneuploidic mosaicisms; -8 [4], -10 [1], -11 [1], -12 [1], -13 [2], -14 [1], -15 [5], -16 [2], -18 [3], -19 [2], -20 [6], -21 [1], -22 [6]; +20 [1] and +22 [1]. In addition, 1 marker chromosome was also observed. Gonosomal chromosome aneuploidic mosaicisms were; -Y [19], -X [4] and + X [1].
The mean values of CAs observed before the procedure, after 24 hours and after 1-3 months are shown in Table 4 and Figure 2.

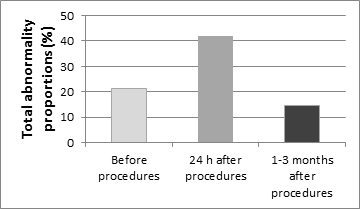
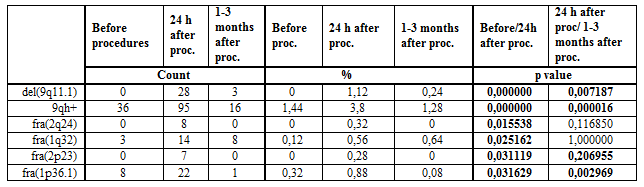
In the patient group, CAs (531/2500) observed before the processing were statistically significant (p=0,000) when compared with the abnormalities (1048/2500) of the subgroup 24 hours after the procedure (181/1250) (p=0,000). Furthermore, the chromosomal damages obtained 24 hours after the processing was compared with that after 1-3 months (181/1250), we found that the damage decreased statistically (p=0,000). Compared CAs of the before the processing and 24 hours after the processing, we found that abnormalities such as fra(1p36.1), fra(1q32), fra(2p23), fra(2q24), del(9q11.1) and 9qh+ (p=0.031629, 0.031119, 0.015538, 0.025162, 0.000000, 0.000000, respectively) were increased statistically (Table 5). This indicates that 1, 2 and 9 chromosomes are more affected than other chromosomes (Figure 1). Moreover, del(9q11.1), 9qh+ and fra(1p36.1) abnormalities were found significantly decreased when compared with 1-3 months after the processing (p=0,007187, 0,000016 and 0,002969) (Table 5).
However, CAs were statistically higher (p = 0,000) in the patients before the processing (18.4%) than the control group (1.5%). For this reason, it was investigated whether patients were associated with CAs before processing with age, gender, smoking, drug use, DM, HT status and CAD. Accordingly, it was seen that there was no statistically significant relation between CAs and these factors (except sex) before the operation (page = 0.25, psmoker = 0.28, pHT = 0.089, pDM = 0.21, pdrug = 0.79, pCAD> 0.05). When CAs and sex of patients were compared before processing, it was statistically determined that CAs were higher in male patients (p = 0.042). It was found that the number of CAs was high in patients receiving high doses and this result was statistically significant (p = 0.042) (Table 6).

4. Findings from radiological workers and control groups
In this group, a total of 17 personnel (6 female and 11 male) working in angiography and radiological procedures and a total of 30 healthy (non-smokers and 17 women and 13 men) with no family history of cancer were compared in terms of CAs as a control group. The age range of the group of personnel was between 27-56, the overall age average was 41.23 ± 6.81 while the age range of the control group was 40-44, and the mean age was 37,13. 850 metaphase cells were analyzed from angiography workers occupationally exposed to the X-ray. Structural and numerical CAs were found in 134 (15.8%) of the cells. The 122 (14,4%) of these damages were structural CAs (5 translocations, 7 deletions, 2 inversions, 2 disentric chromosomes, 17 chromosomal local increases, 70 fragilites, 13 chromatid breaks, 1 chromosomal break, and 5 9qh+). In addition, 12 (1,4%) numerical gonosomal and autosomal aneuploidic mosaicisms were detected (the loss of X chromosome in 5 cells, the loss of Y chromosome in 2 cells, autosomal numerical deviations of -8 [1], -18 [1], -20 [1] and -21 [2]). In the control group, 22 (1.5%) structural CAs were detected in 1500 analyzed cells. All of these CAs were fragilities [fra(2p24), fra(5q31), fra(2q31), fra(6p21), fra(11q22), fra(6q25), fra(2q31), fra(2q13), fra(1q21), fra(1p36.1), fra(4q21), fra(12q24), fra(1q42), fra(1p32), fra(1q42), fra(3q27), fra(5q31), fra(6q23), fra(5q31), fra(2q31), fra(1q21) and fra(2q31)], and all of fragilities was found in 1/50 ratio.
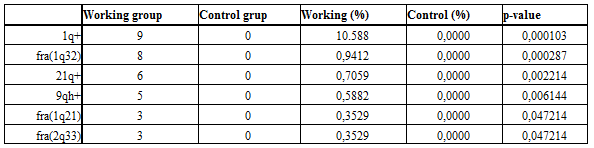
When the total chromosomal damages of the working and control groups were compared; statistically significant difference were found between the two groups (p = 0,000). According to this; the proportion of chromosomal damage in the working group was significantly higher than that of the control group. 1q+, fra(1q32), 21q+, 9qh+, fra(1q21) and fra(2q33) chromosome regions were found statistically higher in the working group (Table 7). Accordingly, it appears that the damages to these 6 chromosomal regions have increased significantly in the radiation exposed personnel.
Diagnostic X-ray procedures are the largest man-made source of IR exposure, and estimation of the risk is difficult. However, IR can be considered as a ‘two-edged sword’ in that it may lead to genetic modifications in exposed, surviving normal tissue. DNA damage is one of the detrimental effects of IR. But, the ability of angiography to produce DNA lesions has yet to be robustly demonstrated. Although many experimental in vitro studies have suggested DNA damage after exposure to X-rays and contrast media, we present in vivo results documenting that angiography scanning in daily clinical routine is associated with increased lymphocyte CAs in this study. But, this is not the first study to suggest that cardiac imaging may be able to cause CAs in peripheral blood lymphocytes tested before and after a IR and contrast media scan.
In the present study; CAs rate was compared with the pre-procedural patients (18.4%) and healthy control group (1,5%); the rate of chromosome damage was found to be very high in pre-procedural patients (p=0,000). The obtained CAs were found to be 68% structural and 32% numerical. The most common damage among these CAs is fragility and this is followed by deletion, translocation, chromatid and chromosome breaks, dicentric and other important structural damages. The fragility may be related to abnormalities in replication, resulting in single-strand DNA gaps, which, if not repaired, may lead to CAs such as deletions within the FS, or translocations or other rearrangements involving breakage at a FS [10]. These findings show that the CAs were significantly higher in cardiovascular patients compared to people who are not exposed to X-rays or healthy control group. Thus, our study found that the overall frequency of CAs was significantly higher in pre-angiography patients compared to the control group. What is the cause of these CAs observed before the patients are exposed to IR and contrast media?
NA damages have been reported to cause the development and progression of CAD [11]. The results of the present study have shown significant increase in genetic damage in lymphocytes of patients with CAD. It has often been reported that genetic damage may be caused by both, extrinsic and intrinsic environments [12]. The 58%, 30%, 48% and 76% of our patients with CAD had hypertension, diabetes, smoking and using drugs, respectively. Hypertension, obesity, hyperlipidemia, stress, smoking, age, sex, and family history are reported to increase risk for
CAD [13]. In our patients before exposed to X-rays, high CAs may be also associated with CAs in risk factors such as smoking, drug use, hypertension, diabetes, stress and age. Indeed, it has been reported that DNA damage in patients with CAD is higher than in controls [14,15]. It had documented that DSBs, oxidized pyrimidines and altered purines were significantly higher in leukocytes of patients with CAD [16]. Oxidative damage increases in aging and age related diseases [17, 18]. However, in some studies; excessive oxidative stress has been reported to play a role in the pathogenesis of cardiovascular disease. Increased production of oxidant free radicals was observed in patients with ischemic heart disease [19]. DNA and CAs can also directly or indirectly stimulate reactive oxygen species, thus providing the basis for cancer formation [20].
A progressive increase in spontaneous chromosome instability/chromosomal loss due to the ageing process is associated with the accumulation of DNA damage due to an age-related decline in DNA repair capacity [20]. Mammalian cells respond rapidly to DNA damage caused by external agents such as IR by rapidly activating the molecular machinery which aims at maintaining genomic integrity and thus preventing carcinogenic mutations. Some studies have found positive association of age with micronuclei acount [21, 22] while others have not [23]. Consequently, individual genetic differences in the ability to repair DNA damage may result in a different susceptibility towards the iodinated contrast agents and, therefore, increase the risk of developing exposure-related disease. The incidence of CAD and diabetes increases especially in people with metabolic syndrome including metabolic disorders such as obesity, hypertension and insulin resistance [17]. Therefore, genetic damages of drugs used in metabolic disorders cannot be ignored. In addition, cardiovascular drugs such as diuretics, beta blockers, calcium antagonists and ACE inhibitors have also been shown to stimulate cancer [24]. Studies have reported that aspirin causes CAs in Chinese hamster ovaries, lung fibroblast cells, and mouse germ cells [25, 26]. The 76% of our patients use drugs (coraspin, beloc, etc.). This suggests that the drugs used by patients may cause genotoxic effects and increase CAs. However, there was no statistical significance between pre-procedural damage and drug use in our study (p = 0.79). The CAs rate in our patients before and 24 hours after treatment was higher in male than in women and this difference was statistically significant (p=0.042). This suggests that X-rays and contrast media may cause more genetic damage in male patients. In one study, it was reported that DNA damage rates in chronic heart patients were not statistically different according to sex [27].
Contrast media is frequently used together with the X-ray in angiography and in interventional radiology. Previous studies have demonstrated that these compounds induce CAs. For this, cytogenetic analysis findings of diagnostic doses of the X rays and contrast media were investigated in experimental studies on cell cultures in vitro [28,29]. Parallel clinical investigations showed an increased genotoxicity in the peripheral blood lymphocytes of the patients undergoing angiography [29-31]. It is well recognized that iodinated contrast media have a cytotoxic effect, and this is felt to be one of the mechanisms responsible for contrast-induced nephrotoxicity [32]. In the present study, patients exposed to the X-rays and contrast media experienced CAs in 30.3% of the cells analyzed after 24 hours. It was found that 73% and 27% of these CAs were structural and numerical mosaicism, respectively. The 43.1% of the structural CAs were found to be fragile, and 18.7% were other significant damages (deletions, chromatid and chromosomal breaks, translocations, dentric, ascentric and marker chromosomes). When compared with the damage observed before the procedures; we found that this was statistically significant (p=0,000), and this significant difference is thought to originate from the X-ray and contrast media.
These findings show that CAs increase significantly in 24 hours after the procedure and that the X-rays and contrast media causes fragility, gaps and breaks on the chromosomes. In fact, it reported that interventional radiological procedures increased CAs in patients after the procedure. DSBs are the most relevant biologic damage induced by IR [34, 35]. The most prominent risk of iodinated contrast agents is nephrotoxicity, rare in patients without a history or symptoms of renal disease. The incidence of kidney injury was 1.3% after percutaneous coronary intervention [36]. Some studies [32, 37, 38] have suggested an association between contrast media and increased DSBs in individuals exposed to low-dose radiation but not necessarily high-dose radiation. The characterization of FS has demonstrated that they are associated with genes that relate to tumorigenesis and behavioural disorders [39, 40]. However, a study has estimated that from 0.6% to 3% of all cancers are due to medical X-rays [41]. It is widely accepted that there is an increased risk of cancer following exposure to IR; this is felt to be most likely due to damage to DNA strands during exposure. Damage to DNA strands can be demonstrated following exposure to X-rays, and new evidence is emerging that this effect may be compounded by administration of iodinated contrast agents. We conclude that application of iodinated contrast media leads to an increase in the extent of DNA damage following irradiation for diagnostic imaging purposes.
In the present study; CAs most frequently seen 24 hours after the procedure; the distribution of damages according to chromosomes appears to be mainly composed of chromosomes 9, 1, 2, X, 5, 3, 6, 4 and 7, respectively, and it was compared with those of the 6 regions on the 3 chromosomes (1p36.1, 1q32, 2p23, 2q24, 9q11.1-q13 and 9qh+) were statistically significant (p=0.031629, 0.031119, 0.015538, 0.025162, 0.000000, 0.000000, respectively). These findings show that chromosomes 1, 2, and 9 are significantly affected by the X-rays and contrast media. Since these chromosome-regions contain innumerable oncogenes, tumor suppressor genes, enzyme genes responsible for DNA repair mechanisms, genes responsible for apoptosis, or candidate genes, these damages may be considered as a risk factor for cancer risk. These overexpressed 1q32, 2q24 and 2p23 chromosome regions decreased significantly in 1-3 months after the procedure, but 1p36.1 region was still highly sensitive (p= 0.002969). This indicates that the damages occurred after 24 hours from the procedure was corrected/repaired at later times. However, it turns out that 1p36.1 region is still unrepairable and sensitive. Most radiation-induced damage is rapidly repaired by various systems within the cell, but DSBs are less easily repaired, and occasional misrepair can lead to induction of point mutations, chromosomal translocations, and gene fusions, all of which are linked to the induction of cancer [9]. It was found that p36.1 and q32 regions on chromosome 1 were the most affected, 24 hours after interventional cardiac procedure, and it was statistically significant (p=0,031629, p=0025,162) in our patients. The chromosome 1 has been reported to contain a large number of tumor suppressor genes in the short arm, leading to the formation of solid tumors. It has also been reported that the 1p36 band is a cancer breakpoint [42]. At the same time, the q24 and p23 regions of chromosome 2 were also significantly stimulated.
In the present study, the most affected chromosomes, by the X-rays, was chromosome 9. These structural chromosomal defects were observed as heterochromatin positive, chromatid and chromosomal breaks, deletions, translocations, inversions and isochromosome. Among these CAs, 9qh+ was the most common. Although this structure is considered polymorphism, clinical outcomes remain uncertain. Despite this uncertainty, our findings suggest that the X-rays and contrast media cause the increase of heteromaterial in the periscentromeric region of chromosome 9. Other structural damages on chromosome 9; 9p and 9q deletions were frequently observed in various malignancies [43-45]. It has been reported that deletions of the 9p are common in melanoma, glioma, leukemia and NSCLC cases [44]. NSCLC patients were reported to have undergone 90% deletion of 9p and breaks between 9q13-9p22 regions [46]. In patients with adenocarcinoma, it has been suggested that the 9q line contains multiple tumor suppressor genes [45]. Consequently, we can easily say that the deletion in the q11.1-q13 region, which is frequently repeated in one of our patients, will play an important role in cancer formation.
Numerous CAs are a common feature of some cancers, suggesting that this is a potent stimulus for tumor development by increasing genomic instability. Our patients have shown that autosomal and gonosomal mosaic CAs are high before and 24 hours after the procedure, and the X-rays and contrast media cause gonosomal mosaicisms (-X and -Y chromosomal monosomes). However, autosomal monozomic mosaicisms (-20, -22, -18, -21, -19) are more common than autosomal trisomic mosaicisms (+21, +2, +8, +18) among autosomal aneuploidic mosaicisms. This also shows that there are sex CAs in the beginning of numerical mosaicisms errors observed in our patients. We can say that increasing numerical sex chromosomes as a result of angiographic procedures can increase sensitivity to tumors. Because, numerical deviations of different chromosomes are reported to be associated with aggressive tumor behavior [47]. Some studies have also shown that structural and numerical sex chromosomal alterations are frequently seen in patients with lung cancer [48, 49]. Thus, numerical deviations of chromosome X have been reported to affect carcinogenesis and poor outcome of different tumor types [50]. One X-chromosome increase has been reported to be relatively common with other karyotypic changes in leukemia, lymphoma, and prostate cancer [51, 52]. In addition, Y chromosome loss has been reported to be common in the cancer cells and several leukemia, papillary renal cell carcinoma, prostate cancer, male chest carcinoma, and pancreatic adenocarcinoma. Further studies have supported the loss of Y chromosome to be a non-phenotypic event related to the aging process in men [53]. Other some studies have shown that age is not clearly related, and that the lost X and Y chromosomes appeared after treatment and in clinical remission. For this reason, it has been concluded that the development of a malignant clone in cancer tissue and the development of sex chromosome loss are more accurate. In men, there is a relationship between bladder cancer and loss of Y chromosome [54]. In addition, Y chromosome loss is common in some cancer types, including pancreatic renal cell carcinoma, and in cancer cells and in some leukemias [55]. All this informations show that numerical sex-chromosome deviations may play a role in the pathogenesis of cancer.
We found that the difference in CAs observed in patient cells analyzed 1-3 months after operation was statistically significant (p=0,000) and the rate of damage significantly decreased when compared 24 hour after the operation. CAs were found in 13.3% of the analyzed cells. The 42% of CAs were found to be fragile, and 15.2% were found to be chromatid breaks, deletions, translocations and disentric chromosomes. Obtained findings reveal that CAs observed before the procedure increased 24 hours after the operation and decreased after 1-3 months. We believe that the reduction in CAs at 1-3 months after the operation has been repaired by DNA repair enzymes and / or damaged cells are destroyed by apoptosis.
Today, interventional cardiologists represent, indeed, the most important group of exposed among professionally exposed physicians. Our study found that the overall frequency of CAs was significantly higher in intermittent personnel working compared to a control group. Workers experienced significant structural damage other than fragility, especially chromatid breaks, inversions and disentric chromosomes. It is seen that the chromosomes 1, 2 and 21 are more affected and damaged in the cells of personnel exposed to radiation. During the imaging process, employees as well as patients are exposed to X rays at significant levels. Exposure to the X-rays of low-dose and long-term or intermittent personnel working in radiological procedures (Physician, Health Technician and Nurse) can prepare the ground for illnesses which may arise after years and can create risks both for patients and employees. It is understood that CAs to working personnel is a consequence of exposure to low dose and long X-rays. The present observations agree with many cytogenetic studies carried out in workers exposed to the X-ray [56-58]. This result also confirms earlier studies [59] that reported a higher frequency of chromatid and chromosome breaks in people occupationally exposed to the X-rays. In a study, it has been reported that chromosomal breaks and disentric chromosomal damages in blood samples of 37 interventional cardiologists are significantly higher than in the control group. In other studies, 50 radiology technicians and control group exposed to long X-rays; it was reported that the radiologist had a mitotic index of 8.2%, leukocyte count of 14,4% and lymphocyte count of 13,3% lower than the control group [58, 60]. Some studies have reported on ring chromosomes in addition to disentric and ascentric chromosomal fragments [56, 61]. In our study, disentric, ascentric and ring chromosome occurrences were found only slightly in the patient and working group. As a result, all these studies show that the elements working in angiography and radiological imaging processes have high genetic damage rates.
The present study demonstrated that before processing, the rate of CAs in patients with CAD was significantly higher than that of the healthy control group. We can say these CAs may be due to cumulative accumulation of internal and external risk factors such as older age, smoking and drug use, diabetes and hypertension. The rate of CAs significantly increased after 24 hours from the operation in patients, indicating that the X-rays used in interventional cardiac radiological procedures and the iodinated opaque material lead to fragilities, gaps, chromatid and chromosomal breaks. In angiography, intravenous iodinated contrast agents can increase DNA damage in addition to radiation. Thus, there is a clear need to evaluate and establish biologic approaches for determining low-dose radiation effects in patients undergoing diagnostic the X-ray procedures. We can say that chromatid and chromosome breaks are very common among structural CAs, the most important primary genetic damage induced by IR, and the predominant indicator of malignancy.
CAs rate in the male patients was higher than the female patient, indicating that X rays caused more genetic damage in male patients. For this reason, male patients need to be more sensitive about radiation. The amount of radiation given to the patients increases as the level of CAs increases. For this reason, the dose of radiation to be given to the patient must be carefully selected. Due to the potentially high genetic damage of patients with CAD, the type and amount of medication to be given and the frequency of radiological diagnostic procedures to be performed should be meticulously adjusted. Patients were observed to have CAs declined significantly after 1-3 months from the operation. This indicates that CAs caused by X-rays and opaque material has been repaired or that damaged cells have been removed by apoptosis. The fact that the extent of such damage may be enhanced by administration of iodinated contrast media will make the imaging community consider in more detail
CAs rate in the male patients was higher than the female patient, indicating that X rays caused more genetic damage in male patients. For this reason, male patients need to be more sensitive about radiation. The amount of radiation given to the patients increases as the level of CAs increases. For this reason, the dose of radiation to be given to the patient must be carefully selected. Due to the potentially high genetic damage of patients with CAD, the type and amount of medication to be given and the frequency of radiological diagnostic procedures to be performed should be meticulously adjusted. Patients were observed to have CAs declined significantly after 1-3 months from the operation. This indicates that CAs caused by X-rays and opaque material has been repaired or that damaged cells have been removed by apoptosis. The fact that the extent of such damage may be enhanced by administration of iodinated contrast media will make the imaging community consider in more detail.
Our findings show that the frequencies of CAs were significantly higher in the interventional cardiologists compared to people who are not exposed to X-rays, and X-rays alone increase genetic damage. Or, interventional cardiologists are likely to receive high radiation exposure as a result of procedures they undertake. For this reason, low-dose and long-term exposure to X-rays of personnel working in radiological procedures (Physician, Health Technician and Nurse) can prepare the illnesses that may arise after years. Therefore, it is clearly necessary to continually monitor both the potential risks and safety of ultrasound exposure. Furthermore, the exact risk at very low doses to a specific individual can be further complicated by many factors, such as carcinogenic agents in our environment, cigarette smoke, diet and genetic back ground. In contrast, exposure to IR may result in adverse health effect on both cardiologists directly and on their progeny. All these informations are in the light; patients should be thought to be more susceptible to DNA damage, depending on the risk factors of CAD, and patients should avoid inappropriate radiological examinations. Physicians and patients should be more careful in this regard, unless X-ray and nuclear imaging techniques are necessary to prevent genetic damage. However, other risk factors other than radiation in CAD should be considered collectively and compared with the risks associated with unidentifiable diseases. İnterventional cardiologists and personnel working have the highest radiation exposure among health professionals.
This work was supported by the Scientific Research Office of Çukurova University (I.U.BAP) (Project no: TYL-2015-5066)
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
